
Featured Course
Limited OB Gyn Ultrasound
The focus of this course is to educate students on the basics of the first trimester scan and the 3rd trimester evaluation.
VIEW TRAINING COURSE
Case Study Details
| Patient Information | |
|---|---|
| Age | 35 |
| Gender | Female |
| Ethnicity | |
| Symptoms (described) | Follow up exam; Previous studies indicated fetus to be small for gestation age and borderline amniotic fluid index. |
| Additional Symptoms (observed) | |
| Health Status | Excellent |
| Evaluation | |
|---|---|
| Prior tests ordered | Limited OB ultrasound to monitor fetal growth |
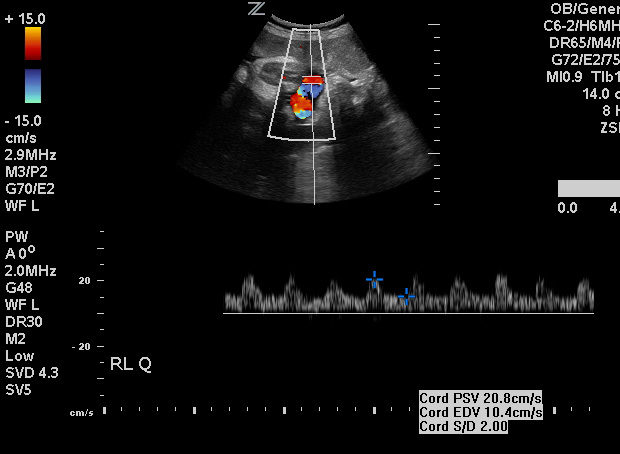
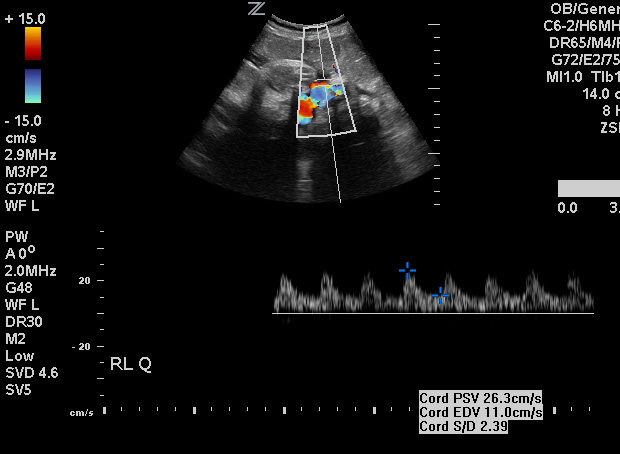
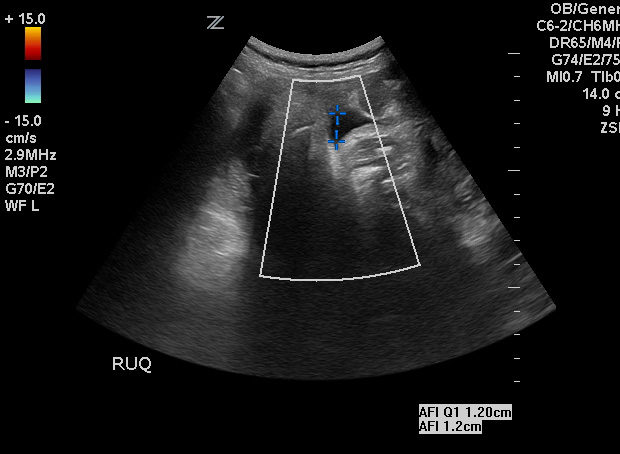
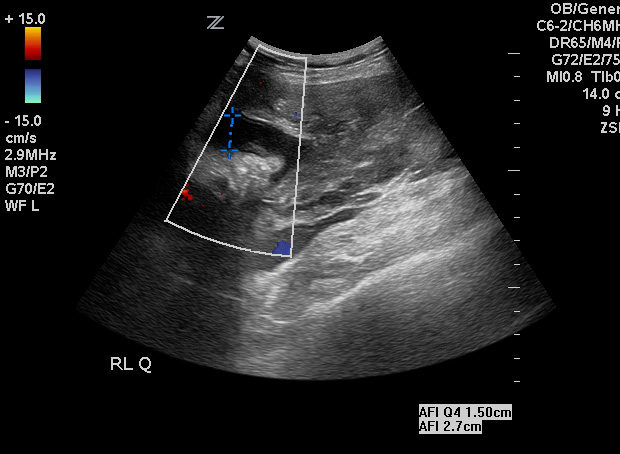
| U/S ordered | Cord Doppler and AFI |
| Additional testing ordered |
| Scanning Protocol | |
|---|---|
| Describe (where, when, how): | Follow up OB ultrasound was performed in the OBGYN’s office. Exam was to monitor amniotic fluid and perform umbilical cord Doppler to assess fetal wellbeing. |
| What equipment was used? | Zonare |
| What technique did you feel was most important for this exam? | Patient should be in a comfortable, supine position. |
| Outcome | |
|---|---|
| Results | Fetal position = vertex. Fetal heart rate = 146; Low AFI = 2.5cm; Cord Doppler = S/D ratio 2.0 and exhibited diastolic flow. |
| Note | Due to the low AFI, patient was scheduled cesarean delivery at 5pm that evening |
| Diagnosis | IUGR; Oligohydramnios |
Cesarean delivery
Mother tolerated procedure well and is making an excellent recovery. Baby suffered respiratory problems, due to immature lung development, and low muscle tone. Baby is currently in the Neonatal Intensive Care Unit. He has been removed from the respirator and is breathing room air. But is undergoing physical therapy for muscle tone and sucking development.
Tell Us Your Story
We want to hear how you are using Ultrasound to improve patient care. Email Us Your Story